What Are Fibroids?


The term “fibroids” is often used to refer to abnormal growths that are found in or on the uterus. Also known as uterine fibroids or uterine leiomyomas, they originate from the smooth muscle and connective tissue of the uterine muscle. It is the commonest tumor affecting the reproductive organs. They are generally benign and can be attributed to a monoclonal proliferation of the smooth muscles.
The severity of the symptoms often depend on the location, number, and size of the fibroids. In some cases, it may even be asymptomatic. There is a genetic predisposition to uterine fibroids. It most commonly affects women in the reproductive age group with an estimated incidence of more than 70% by 50 years of age.

1. Pathophysiology
Fibroids are generally round and well circumscribed nodules that are solid and white or tan in color. When sectioned or cut, it may show a whorled appearance. Although the size of fibroids may vary, most fibroids are usually the size of a grapefruit or bigger and can be felt through the abdomen. Fibroids are monoclonal tumors. Although not clearly understood, it is postulated that fibroids are caused by genes, prenatal hormone exposure, growth factors, hormone effects, and xenoestrogens. Estrogen and progesterone is believed to have a mitogenic effect on the fibroid cells. It is believed that estrogen increases the growth of fibroid cells by up-regulating factors such as the insulin-like growth factor 1 (IGF1) and epidermal growth factor receptor (EGFR).

2. Classification
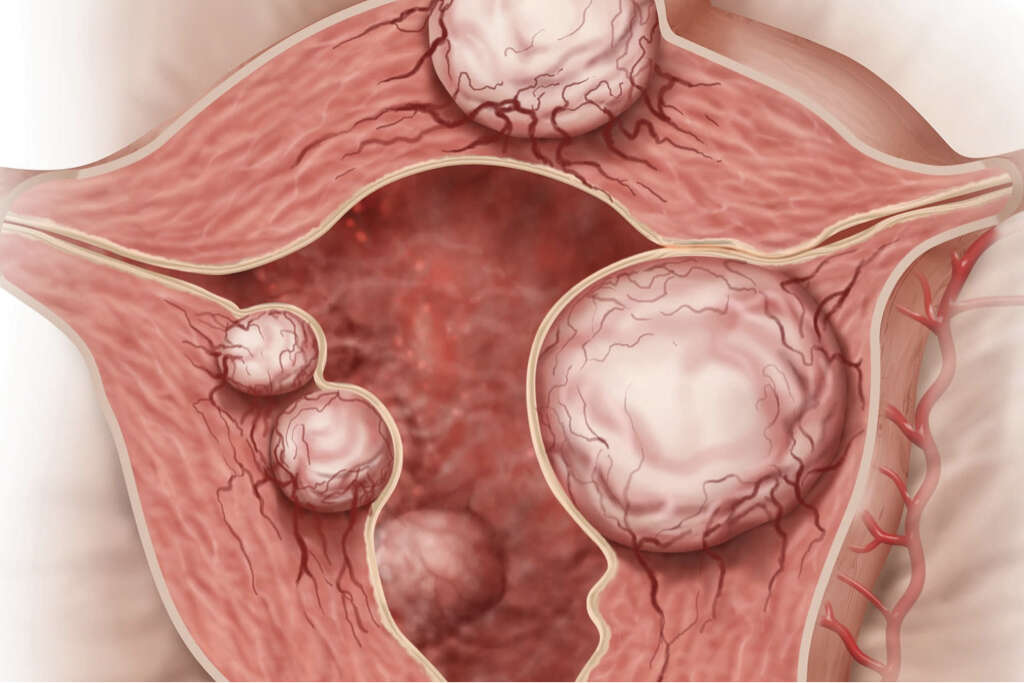
The symptoms and its severity depends on the growth and location of the fibroids. For example, a large fibroid on the outside of the uterus may cause less issues than a small fibroid in the uterus. Fibroids can be classified based on their location. Subserosal fibroids are on the surface of the uterus and grow outward from the surface.
Intramural fibroids are found within the uterine wall. This is the commonest type. Most are asymptomatic unless they are large in size. They may eventually grow inward and distort the uterine cavity. Submucosal fibroids are found in the muscle closer to the inner surface of the uterus. These fibroids easily distort the uterine cavity and small lesions can cause infertility and bleeding. Cervical fibroids are those found in the cervical wall.
3. Statistics
By the age of 50 years old, it is estimated that 20% to 80% of women develop fibroids. In 2013, it was estimated that about 171 million women were affected globally. Fibroids are usually found in the middle and reproductive years for women. Once they reach menopause, the fibroids generally start to decrease in size.
A study has observed that surgery to remove uterine fibroids are more common among women with “higher social classes.” Although fibroids are common, up to 50% of those affected are asymptomatic. In the United States, about 80% of African American women will develop benign fibroids by their late 40s. Fibroids are more common among African American women compared to Caucasian women. They also tend to grow faster, occur at a younger age, and are more likely to cause issues resulting in higher surgical rates.

4. Risk Factors
Some of the risk factors of fibroids are obesity and being in the reproductive years, as fibroid growth is dependent on estrogen and progesterone. Dietary choices also play a role as a diet that is high in vegetables and fruits may reduce the risk of developing fibroids.
Some say that having normal dietary levels of vitamin D can decrease the risk of fibroids. About 50% of uterine fibroids have a genetic abnormality. When a woman has fibroids, the risk of her daughter having fibroids is three times higher than usual. Women of African descent have 3 to 9 times higher risk of developing uterine fibroids compared to Caucasian women. Reed’s syndrome can cause uterine fibroids, cutaneous fibroids, and renal cell cancer. This is due to the gene mutation that produces an enzyme known as fumarate hydratase.

5. Signs and Symptoms
As previously mentioned, about 50% of women with fibroids have no symptoms. The symptoms also depend on the location and size of the fibroid. Some of the signs and symptoms of women with fibroids are anemia, menorrhagia (increased menstrual bleeding), abnormal bleeding (bleeding between cycles), abdominal pain, pain during intercourse, and difficulty conceiving.
Some women may also be able to feel a lump in the abdomen. During pregnancy, fibroids can also increase the risk of miscarriage, premature labor, bleeding, and interfering with the positioning of the fetus. When the size of the fibroid becomes large, it can mimic a pregnancy or extend outward through the cervix and vagina. Although a potential cause of infertility, most women will have normal pregnancy outcomes.
6. Diagnosis
When the diagnosis of a uterine fibroid is suspected via the patient’s history and a physical examination, an ultrasound can be used to identify the lesion. The ultrasound will help to determine the location and size of the fibroid. This can be better defined using a magnetic resonance imaging (MRI) scan. It is important to rule out other conditions such as an adnexal tumor or an ovarian tumor.
Although imaging cannot clearly distinguish between a benign uterine fibroid and malignant uterine leiomyosarcoma, the malignant version is quite rare. There should be suspicion of a sarcoma when there is rapid or unexpected growth and enlargement of the fibroid after menopause. If malignant, imaging may show local invasion. Other tests that may be beneficial are sonohysterography and hysterosalpingography.
7. Coexisting Disorders
There may be some coexisting disorders with uterine fibroids. When it causes heavy bleeding, it can cause anemia and iron deficiency. Patients with these issues are generally pale and tired. A complete blood count (CBC) can easily determine if anemia is present. Large fibroids can cause pressure effects such as abdominal bloating and constipation.
This is due to the pressure exerted by the fibroid on the rectum. A large fibroid also increases intraabdominal pressure. Compression of the ureter (tube connecting the kidneys and bladder) can result in hydronephrosis (dilation of the kidneys due to backflow of urine). Fibroids can also occur concurrently with endometriosis and adenomyosis. In rare cases, cancerous growths may occur.

8. Medical Care
There are several medications that can be used to control the symptoms of fibroids. Nonsteroidal anti-inflammatory drugs (NSAIDs) can help to reduce pain. Uterine bleeding and cramps can be reduced using oral contraceptive pills. Patients with anemia will benefit from iron supplementation. Cabergoline and Danazol may help reduce the size of the fibroids.
Ulipristal acetate has also shown promise in fibroid size reduction by up to 70%. Gonadotropin releasing hormone analogs may help reduce fibroid size but is rarely prescribed due to the side effects of the medication. Progesterone antagonists (such as mifepristone) and aromatase inhibitors may also be beneficial. Levonorgestrel intrauterine devices can be inserted into the uterus to help decrease menstrual flow and improve other symptoms.

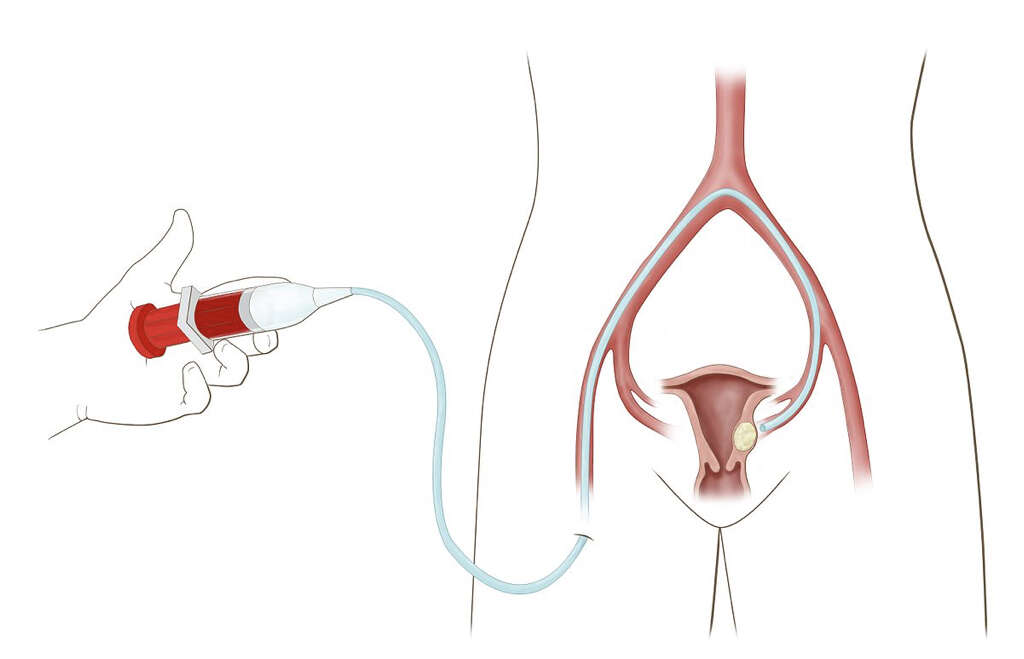
9. Surgical Care and Other Procedures
Uterine artery embolization (UAE) is a procedure that can be used to block blood flow to the fibroid, resulting in reduced size. Although noninvasive, there is some evidence that shows more repeat procedures may be required. Uterine artery ligation is a similar procedure where surgery is performed to limit the blood supply of the uterus. A myomectomy is a surgery to remove the fibroids.
It is generally only recommended when conservative treatment fails or for women who want to preserve their fertility. The National Institute of Clinical Excellence has guidelines stating that a UAE and myomectomy have the potential to retain fertility. Other surgical procedures that may be performed include a hysterectomy (removal of the uterus), endometrial ablation, and radiofrequency ablation.
10. Prognosis and Research
Although most uterine fibroids are benign, it is estimated that about 1 in 1,000 lesions are or become malignant. These malignant lesions are usually a leiomyosarcoma. Some of the factors to look out for include increasing growth of fibroids after menopause, rapid growth, or unexpected growth. When malignancy is suspected, surgical treatment is recommended.
One study comparing the effect of an aromatase inhibitor (letrozole) against a gonadotropin releasing hormone agonist therapy (triptorelin) found that the size of the fibroid was reduced by 45.6% in the letrozole and 33.2% in the triptorelin group. In this study, no women taking letrozole reported hot flashes while all women taking triptorelin experienced hot flashes. This led the researchers to conclude that aromatase inhibitors can be used to manage fibroids without causing significant changes in the hormone levels.